Dr. Kerri Winters-Stone and Dr. Jacob Raber from Oregon Health and Science University, describe a research paper they co-authored that was published by Oncotarget in Volume 13, entitled, “Association of fall rate and functional status by APOE genotype in cancer survivors after exercise intervention.”
Behind the Study is a series of transcribed videos of researchers elaborating on their oncology-focused research published by Oncotarget. Visit the Oncotarget YouTube channel for more insights from outstanding authors.
—
Hi, I’m Kerri Winters-Stone from Oregon Health and Science University, and I’m here with my colleague, Dr. Jacob Raber, to talk about our paper, “Association of fall rate and functional status by APOE genotype in cancer survivors after exercise intervention.”
The number of cancer survivors in the US is increasing exponentially. In 2022, there were approximately 17 million cancer survivors in the US, and our healthcare system is largely unprepared to meet the needs of this population, most of whom are older and have additional health risks related to their cancer. Together, both cancer and aging pose many threats for our older survivors. In addition to the age-related declines that they’re already experiencing, cancer treatment can accelerate aging, leading to higher levels of weakness, mobility problems, muscle loss, that together cause an increased rate of falls that can accelerate the risk of fracture.
To address this problem, we conducted a study called GET Fit. This was a fall prevention trial to try and reduce falls in women who were treated with neurotoxic chemotherapy. GET Fit is an NIH funded trial and is registered at clinicaltrials.gov. It’s a three arm randomized controlled trial comparing well recognized age-related fall prevention exercise approaches to reduce the falls that we think are related to chemotherapy in women treated for cancer. We aim to recruit 456 women, ages 50 to 75 with a history of chemotherapy who are currently underactive. And eligible women were randomized to a group that either performed six months of supervised group Tai Ji Quan, or more familiarly Tai Chi, exercise, or to a group that performed lower body strength training, or to our placebo control group that performs seated stretching exercise. So women engage in those groups for six months and then we conduct an additional six-month follow up. Our primary endpoint were self-reported falls, and secondary endpoints were fall related injuries, muscle strength, and postural stability.
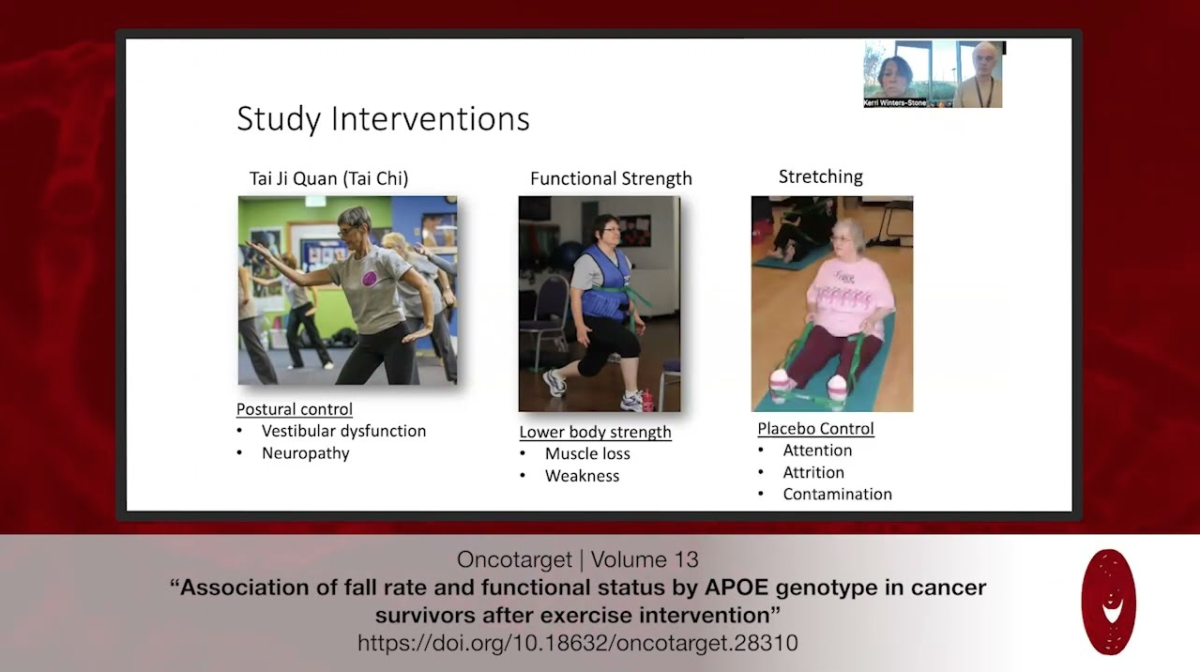
Briefly, our study interventions, Tai Ji Quan, is aimed to improve postural control that we believe may be affected by vestibular dysfunction and neuropathy resulting from chemotherapy. A functional strength training program is designed to address muscle loss and weakness that accompanies chemotherapy as well as deconditioning during cancer treatment. And then our stretching control group is a seated stretching group that is designed to not improve postural stability, nor to improve muscle strength, but rather provide equal amounts of attention to control for attrition as well as contamination.
We were able to enroll 460 women into the GET Fit trial and here are their baseline characteristics. 442 women were allocated to groups and received the intervention. Women were in their lower 60s. The majority of participants were Caucasian and they were relatively healthy and within about five months of their cancer diagnosis. 21% of the sample had a fall history at baseline, 37% of those fallers were recurrent fallers. And overall, we retained 88% of the sample throughout the 12 month study, and adherence to the exercise programs averaged 73%.
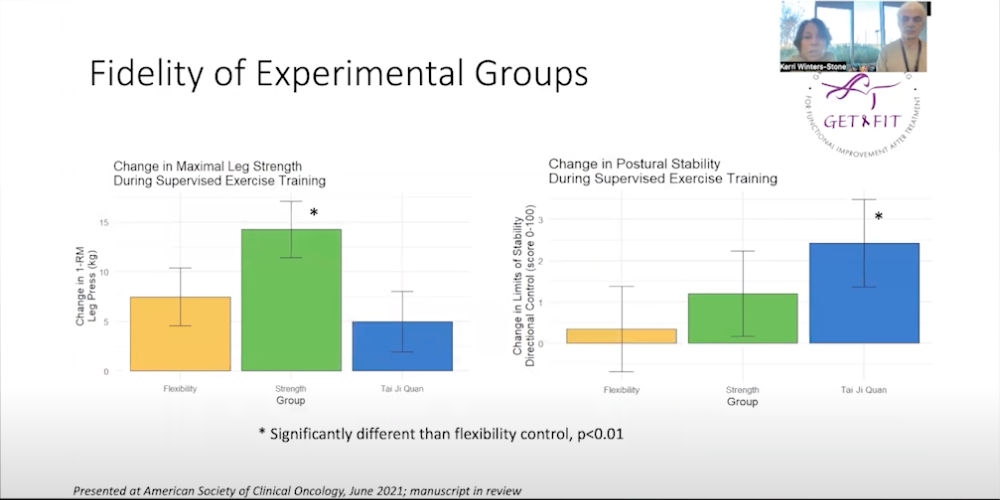
These graphs show the fidelity of our experimental groups. You can see on the left hand side that changes in maximal strength were significantly greater in the group assigned to the strength training program compared to Tai Ji Quan or flexibility control. And on the right hand side, changes in postural stability were significantly more improved in women assigned to the Tai Ji Quan group compared to the strength or flexibility control groups.
This graph shows the incidence density for injurious falls. We did not observe a reduction in falls or injurious falls across the experimental groups, but when we compared the groups to their baseline fall history, we observed a 45% reduction in injurious falls from baseline fall rates within the tai ji quan group. Now I’ll hand it over to Dr. Raber.
Yeah. I’m Jacob Raber and I was very excited to start collaborating with Dr. Winters. We are very interested in apolipoprotein E in human isoforms, E2, E3 and E4, and compared to E3, which is most common. APOE4’s the risk factor for cardiovascular disease and Alzheimer’s disease, and also, cognitive impairments for environmental challenges including also cardiac bypass surgery. So question is, thinking about the interventions that Dr. Winters just explained, if you have a certain APOE genotype, would one intervention work better for you than another one?
So here you see, first of all, risk to develop Alzheimer’s disease based on APOE genotype. So you see here, one is the E3/E3 homozygous, and you can see at age 65, which is about the peak age of risk to get Alzheimer’s disease, the E4/E4 carriers have a 15 fold increased risk.
Now, as you can see on the next slide, there is also a sex difference in this risk. So women with E4/E4 have a higher risk to develop Alzheimer’s than men with E4/E4, and the same is for E3/E4 in women compared to men.
So on the next slide, I want to give you one example. Here you see on the left strength training. So you see we divided the population in those that carry APOE2 and those who do not, compared to APOE3 protective in terms of risk to develop Alzheimer’s disease. And you can see here that the E2 carriers, they see more symptoms after the intervention compared to the non E2 carriers, and it is both baseline intervention as well as post intervention.
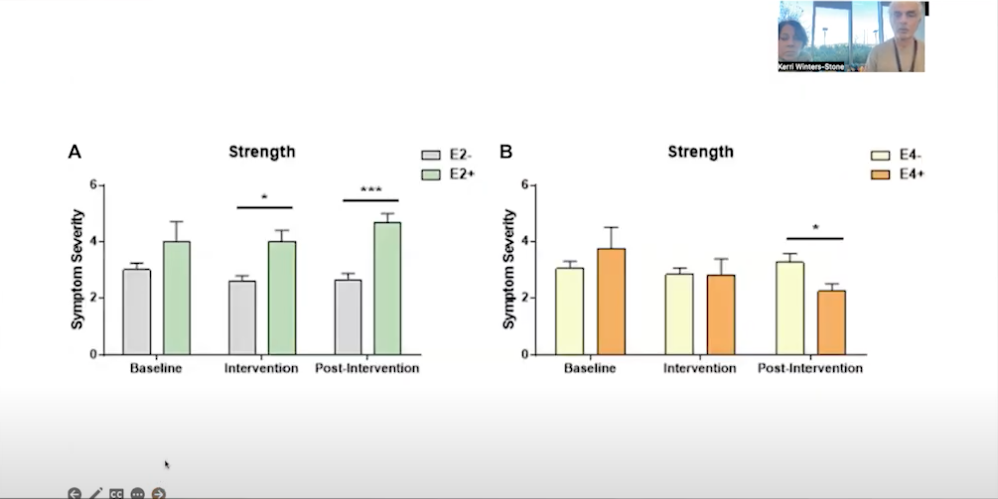
Now, on the right panel, you see that it’s actually the opposite for the E4 carriers. The E4 carriers, post intervention, they show less symptoms. So they benefited more from the strength intervention than the non E4 carriers. So clearly, your APOE genotype modulates the response to the exercise intervention.
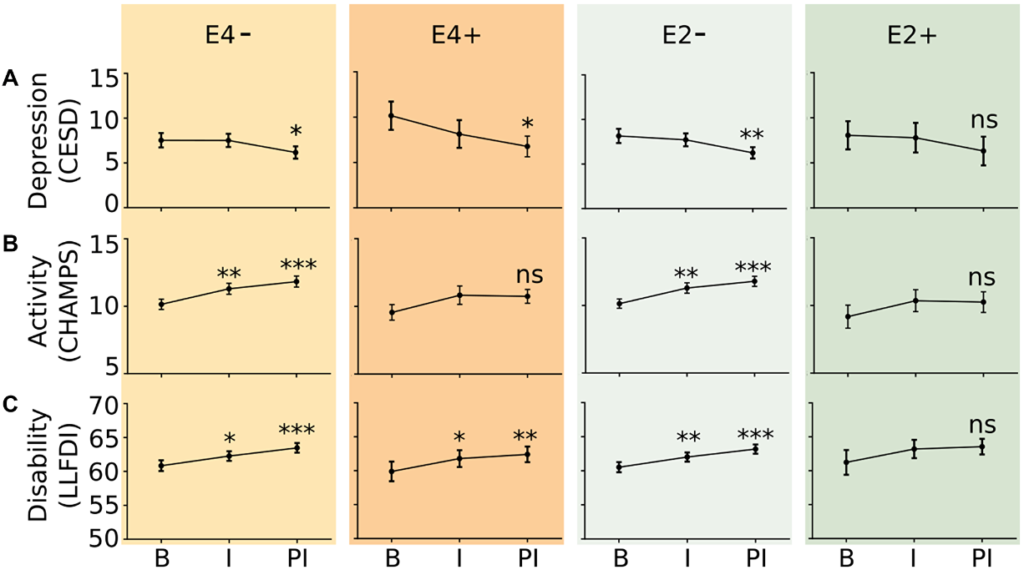
So here you see the results and conclusions. So we had 126 female cancer survivors, and E4 carriers tended towards a higher fall rate at baseline. But after exercise intervention, they had a lower fall rate compared to non E4 carriers, both immediately after structured intervention as well as six months after follow up. E2 carriers did not show improved measures of depressive symptoms and self-reported disability after exercise intervention. E3 homozygotes showed increased self-report physical activity after the six months exercise intervention, but E4 and E2 carriers did not. So APOE genotype may modulate cancer treatment related side effects and symptoms as well as response to exercise intervention.
So it’s important to determine whether this APOE genotype-dependent exercise response we see here is relevant to other cancers as well. And Dr. Winters and I are planning for those kind of studies.
Click here to read the full study published by Oncotarget.
ONCOTARGET VIDEOS: YouTube | LabTube | Oncotarget.com
—
Oncotarget is a unique platform designed to house scientific studies in a journal format that is available for anyone to read—without a paywall making access more difficult. This means information that has the potential to benefit our societies from the inside out can be shared with friends, neighbors, colleagues and other researchers, far and wide.
For media inquiries, please contact media@impactjournals.com.