Dr. Mangesh A. Thorat from Guy’s Hospital in London, Queen Mary University of London, and King’s College London, describes a recent editorial he authored that was published by Oncotarget in Volume 14, entitled, “Multiclonality of ER expression in DCIS – Implications for clinical practice and future research.”
Behind the Study is a series of transcribed videos of researchers elaborating on their oncology-focused research published by Oncotarget. Visit the Oncotarget YouTube channel for more insights from outstanding authors.
—
Hello, greetings from London. I’m Dr. Mangesh Thorat. I work at the Guy’s Hospital as a Locum Consultant Oncoplastic Breast Surgeon, as well as at Queen Mary University of London, and King’s College London as an Honorary Senior Lecturer.
Today, I’m going to talk about my paper titled, “Multiclonality of ER expression in DCIS – implications for clinical practice and future research,” published in the Oncotarget.
The paper discusses important aspects of our work on estrogen receptor expression in ductal carcinoma in situ that is DCIS. The key reason to undertake this research was that the role of commonly used prognostic and predictive biomarkers in the invasive form of breast cancer was under-investigated in DCIS, and the published data were inconclusive. This was a major weakness that stopped us from personalizing treatment for DCIS patients. Therefore, we decided to address this unmet need.
As someone originally coming from low resource setting, I was also keen that the biomarkers we investigate in this research project should be based on acid methodology that is easily available in average pathology labs across the world. This way, if prognostic or predictive role of a biomarker is proven, then it can be implemented anywhere in the world. As a result, we chose to focus on immunohistochemistry as the main assay methodology.
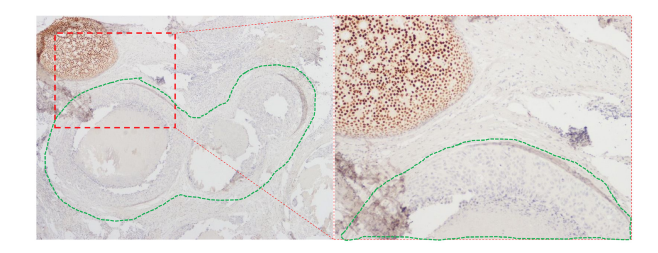
When I started scoring the ER immunohistochemistry slides, I observed that some of the otherwise ER positive DCIS that is already scored three or more on whole sections, also contain carcinoma and situ ducts that completely lacked ER expression. This admixture of clearly ER positive and ER negative ducts is not the same as heterogeneity in ER expression, and I labeled such DCIS cases as multiclonal DCIS, even if just one carcinoma in situ duct in the entire section lack ER expression.
What we observed when we analyze the data, was that even though these multiclonal cases currently get classified as ER positive DCIS, they actually behave exactly like ER negative DCIS. That is, the ER negative clone within that DCIS is the dominant clone that determines the outcome. We found that ER is a strong prognostic biomarker in DCIS, but more importantly, it is an even stronger biomarker if we rectify the current misclassification of multiclonal cases and classify them as ER negative, as per our proposed clonal method.
What we would like to do next is we aim to investigate genomic variation and similarity between these different clonal populations within the same DCIS and also compare it to the recurrences where a matching recurrence is available.
Meanwhile, the important practice implication is that ER should be routinely evaluated in DCIS and the method employed should be the clonal method we have described. I have also discussed the research implications of our findings in the paper.
But one important point I would like to emphasize here for this research: I was a surgeon looking down the microscope and probably the first surgeon to have seen such multiclonal expression of ER in DCIS, but I’m sure that many pathologists would’ve observed it before. The difference in this case, however, was that I decided to systematically pursue this simple clinical observation with an open mind and inclusiveness, and this has given us valuable insights. It underscores the importance of systematically pursuing simple observations, even in today’s era of high-tech research. I firmly believe that these will still provide meaningful insights.
I would like to thank our collaborators and colleagues for their support in this work, as well as Cancer Research UK and Breast Cancer Research Foundation of New York for their funding support. Thank you for listening to my few words.
Click here to read the full editorial published by Oncotarget.
—
Oncotarget is a unique platform designed to house scientific studies in a journal format that is available for anyone to read—without a paywall making access more difficult. This means information that has the potential to benefit our societies from the inside out can be shared with friends, neighbors, colleagues and other researchers, far and wide.
For media inquiries, please contact [email protected].